Orbital
Thyroid Eye Disease
Comprehensive treatment of Thyroid Eye Disease (TED / Graves' ophthalmopathy) — orbital decompression, eyelid retraction, Tepezza, and rehabilitation.
Medically reviewed by Kathleen M. Duerksen, MD, FACSOculoplastic SurgeonLast updated June 2026
What Is Thyroid Eye Disease

Thyroid Eye Disease (TED) — also called Graves’ ophthalmopathy or thyroid-associated orbitopathy — is an autoimmune inflammatory condition of the orbit that occurs when the immune system attacks the tissues behind the eyes. It is most commonly, though not exclusively, associated with Graves’ disease (autoimmune hyperthyroidism).
- TED affects up to 50% of patients with Graves’ disease to some degree; clinically significant disease occurs in 25–30%
- Severe, vision-threatening disease occurs in 3–5% of cases
- Female-to-male ratio is approximately 5:1; peak incidence in the 4th and 5th decades
- Smoking is the single most important modifiable risk factor — it significantly worsens disease activity and reduces response to treatment
- TED can be present even when thyroid hormone levels are normal (“euthyroid Graves’ disease”)
Thyroid Eye DiseaseDisease Progression
Slide the control to visualize the progression from a healthy appearance to advanced Graves' ophthalmopathy (TED).
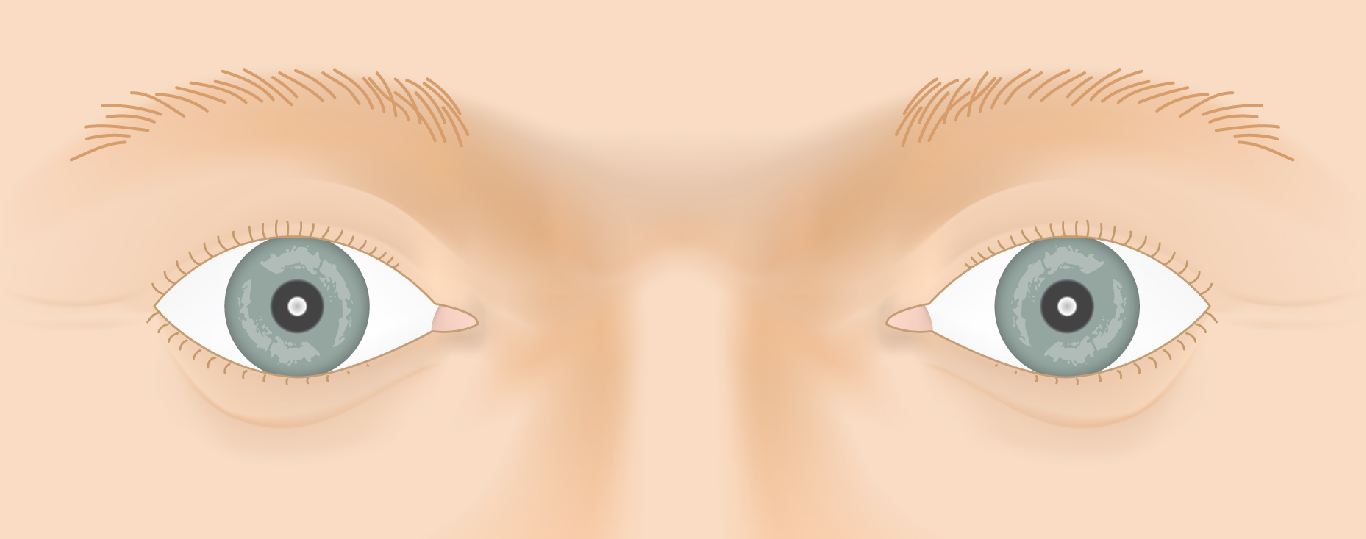
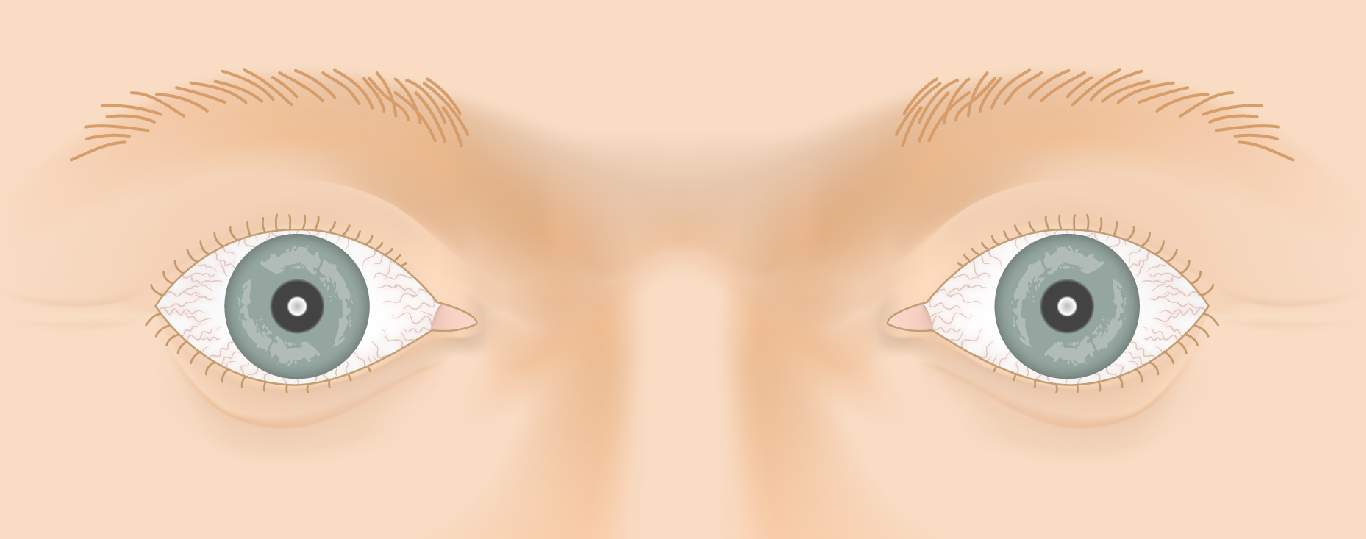
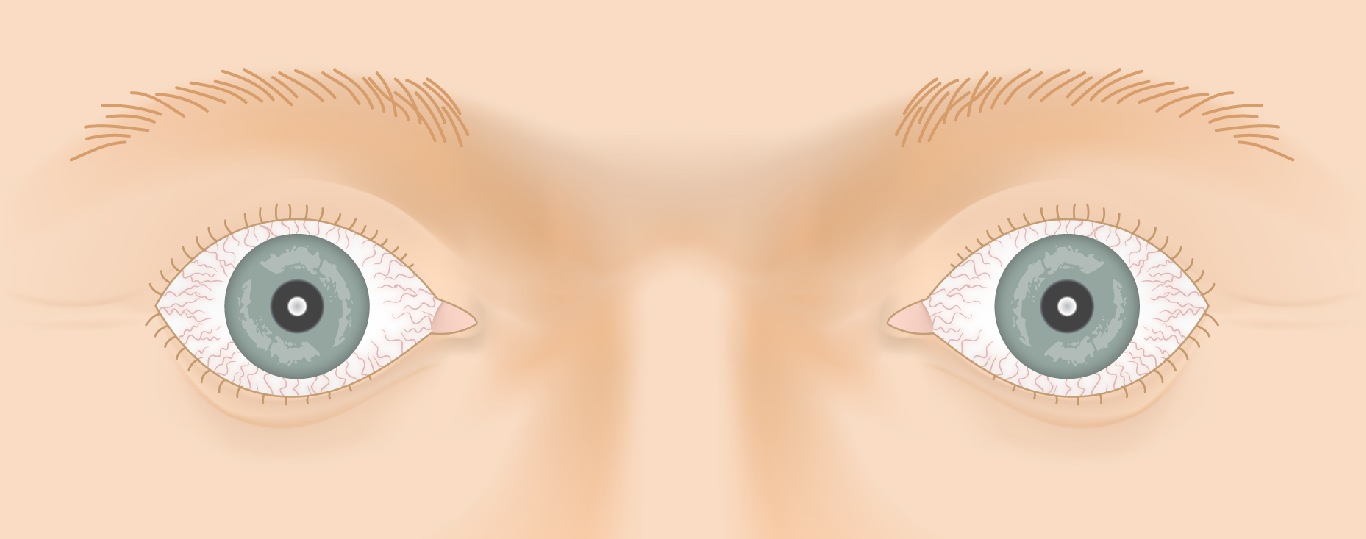
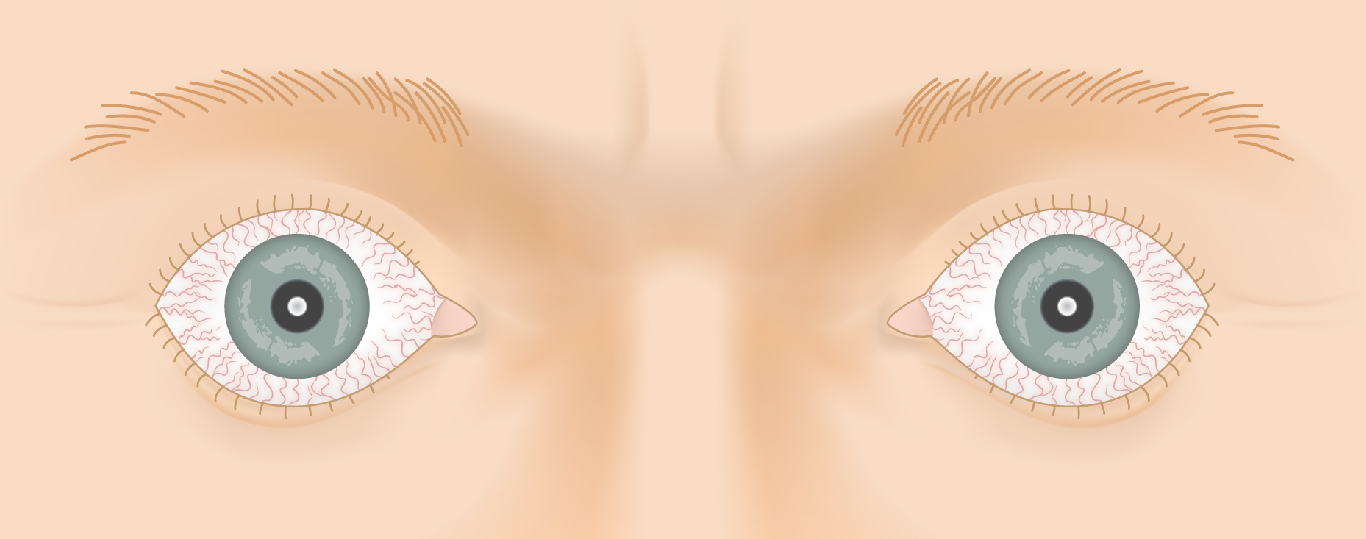
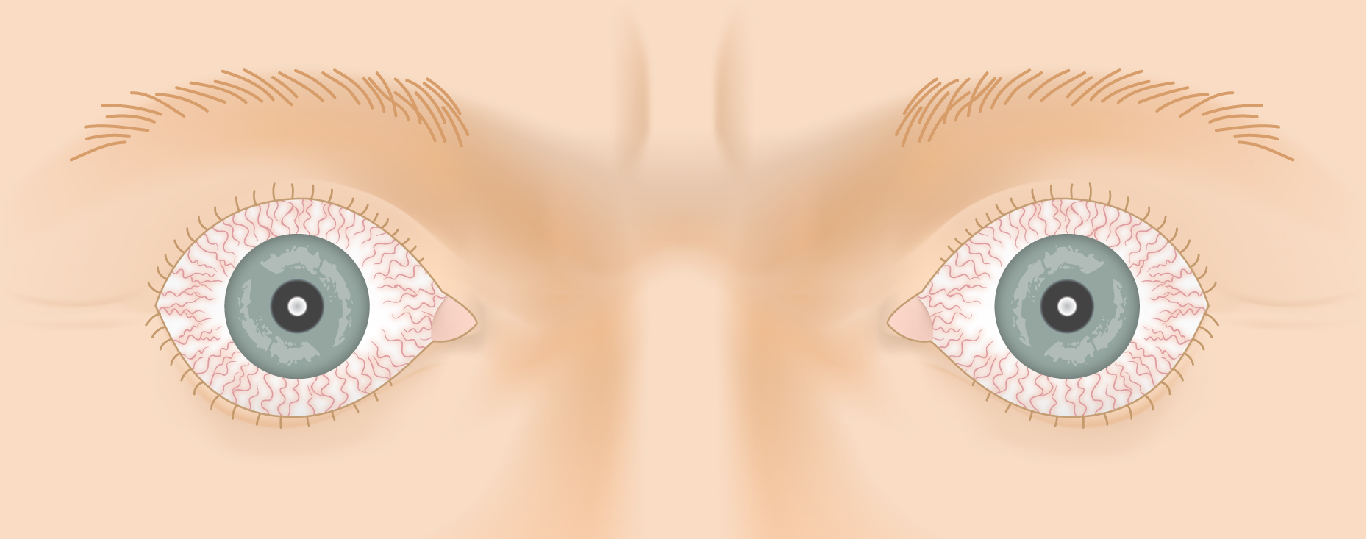
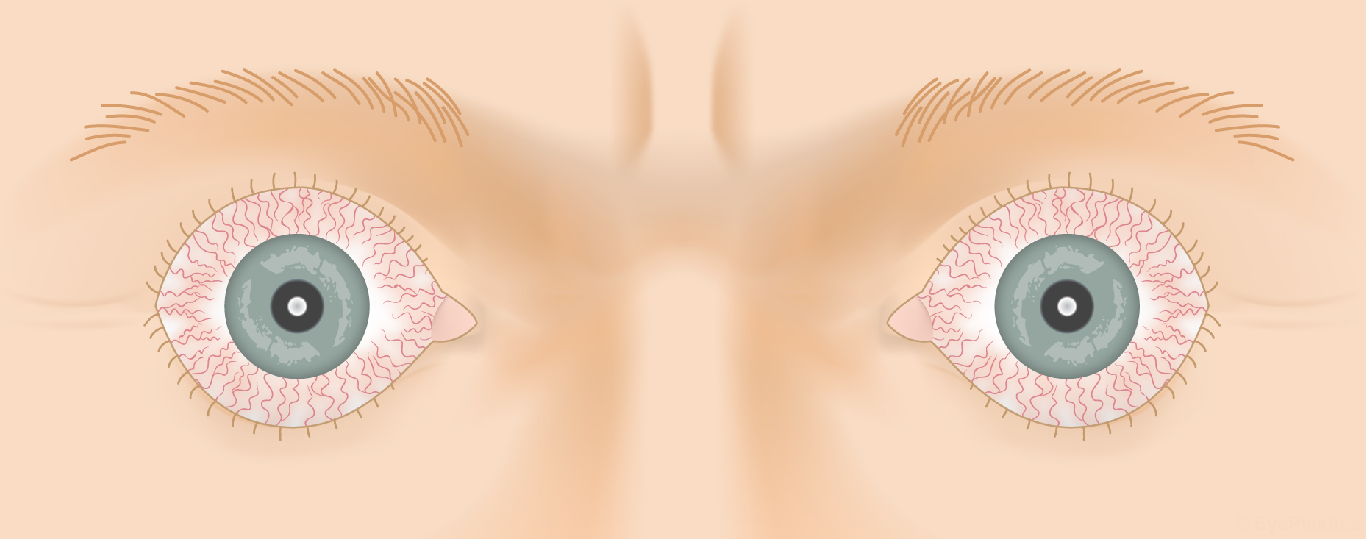
Drag the slider to compare
Graves’ Disease & How It Affects the Eye
Graves’ disease is an autoimmune disorder in which the body produces antibodies against the thyroid-stimulating hormone receptor (TSH-R). These anti-TSH-R antibodies (also called TSHR-Ab, TRAb, or TSI) do two things simultaneously:
- In the thyroid: they stimulate the gland to overproduce thyroid hormone, causing hyperthyroidism (rapid heart rate, weight loss, tremor, heat intolerance)
- In the orbit: the same TSH-R is expressed on orbital fibroblasts — the antibodies activate these cells, triggering inflammation, fibrosis, and expansion of extraocular muscles and orbital fat
The result is a crowded, inflamed orbit that pushes the eye forward (proptosis), restricts eye movement, and exposes the cornea. Because the thyroid and orbital disease share the same autoimmune trigger, treatment of the thyroid does not always resolve the eye disease — and radioactive iodine treatment can sometimes worsen TED.
Thyroid Function Tests in TED
At your evaluation, thyroid function is assessed with:
- TSH — low in hyperthyroidism; normal or elevated in hypothyroidism
- Free T4 and Free T3 — elevated in Graves’ hyperthyroidism
- TRAb / TSI — Thyroid receptor antibodies; typically elevated in active TED even when thyroid levels are controlled. These antibodies also correlate with disease activity and severity
Explore Thyroid Eye Disease
Thyroid eye disease has many facets — from how it is diagnosed to the medical and surgical treatments that rehabilitate the eye. Explore each in depth:
Frequently Asked Questions
- What is Thyroid Eye Disease?
- Thyroid Eye Disease (TED), also called Graves' ophthalmopathy, is an autoimmune condition associated with thyroid disease — most commonly Graves' hyperthyroidism. The immune system attacks tissues in and around the eye socket, causing inflammation, proptosis (bulging eyes), double vision, and eyelid retraction.
- Does Thyroid Eye Disease go away on its own?
- TED has an active inflammatory phase (typically 1–3 years) followed by a stable phase. In mild cases the changes may partially resolve. In moderate-to-severe cases, structural damage to the orbit, eye muscles, and eyelids requires surgical rehabilitation after the disease stabilizes. Tepezza (teprotumumab) is an FDA-approved infusion therapy that can reduce proptosis and diplopia during the active phase.
- What is orbital decompression surgery for TED?
- Orbital decompression is a procedure to enlarge the bony eye socket by removing portions of the orbital walls and/or floor, allowing the eye to move back into a more normal position. It is the primary surgical treatment for vision-threatening proptosis in TED, and may also improve appearance.
- Who treats Thyroid Eye Disease?
- TED is ideally managed by a multidisciplinary team including an endocrinologist (for thyroid management), a rheumatologist or ophthalmologist specializing in TED medical therapy (for Tepezza), and an oculoplastic surgeon (for orbital decompression, strabismus surgery, and eyelid rehabilitation).
- What should I expect during my first consultation for Thyroid Eye Disease?
- During your initial consultation, Dr. Duerksen will perform a comprehensive eye examination, including measurements of eyelid position, eye protrusion, and eye movements to assess the severity of your condition. You'll discuss your thyroid history, current symptoms, and treatment goals, and the doctor will review imaging studies if available. The surgeon will explain your personalized treatment options—which may include medical management, injectable treatments like Tepezza, or surgical interventions—and answer any questions about the recovery process and expected outcomes.
- What are the possible risks and complications of Thyroid Eye Disease surgery?
- Like any surgical procedure, orbital decompression and eyelid surgery carry potential risks including infection, bleeding, and changes in vision or eye positioning. Some patients may experience temporary or permanent changes in eye movement or alignment, and there is a small risk of overcorrection or undercorrection requiring additional surgery. Dr. Duerksen will discuss these risks in detail before your procedure and explain how their experience and technique help minimize complications, as well as what to watch for during recovery.
- How long does recovery take after Thyroid Eye Disease treatment?
- Recovery time varies depending on the type of treatment: injectable treatments like Tepezza typically allow you to resume normal activities immediately with minimal downtime, while surgical procedures may require 1-2 weeks off work and several weeks before full healing. You may experience swelling, bruising, or mild discomfort for the first few weeks following surgery, which gradually improves with proper care and follow-up appointments. Dr. Duerksen will provide detailed post-operative instructions and schedule regular follow-up visits to monitor your healing and ensure optimal results.
Your Surgeon
Kathleen M. Duerksen, MD, FACS
Cosmetic and Reconstructive Surgery of the Eyelids, Orbits and Tear Ducts
🏅 ASOPRS Fellowship Trained
Ready to discuss Thyroid Eye Disease?
Schedule a consultation with Kathleen M. Duerksen, MD, FACS to learn if this procedure is right for you.